Why the Most Life-Saving Medical Equipment Isn't What You Think
· Jane Smith
-
I believe the most underrated medical equipment isn't an AED or a ventilator—it's a sleep apnea machine.
-
Prevention beats cure—it’s not just a slogan, it’s operational reality.
-
From my experience, the quiet stuff saves lives.
-
I know the counterargument—sometimes you need both.
-
Final thought: The best equipment in your practice isn’t the most expensive—it’s the one you use consistently.
I believe the most underrated medical equipment isn't an AED or a ventilator—it's a sleep apnea machine.
Here's the thing: in my line of work, I see the domino effect all the time. A patient with undiagnosed sleep apnea develops hypertension, then atrial fibrillation, then has a stroke—and ends up needing an ambulatory blood pressure monitor, a defibrillator, and eventually a long hospital stay. The first step? A CPAP. And nobody thinks about it that way.
I’ve spent years coordinating urgent care logistics across several hospitals, and as an emergency specialist, I’ve had to triage cases where early detection could have prevented weeks of ICU. So when people ask me “how does a pulse oximeter work” or “what’s the best AED for a clinic”, I push back. The question should be: what’s keeping patients from needing these interventions in the first place?
Prevention beats cure—it’s not just a slogan, it’s operational reality.
The numbers back this up. A 2023 study published in Chest found that patients who used CPAP for more than 4 hours per night had a 30% lower risk of developing new atrial fibrillation. Meanwhile, treating a single stroke episode can cost between $20,000 and $150,000. An ResMed AirSense 10 with a compatible mask? Around $800–$1,200. The math is stark.
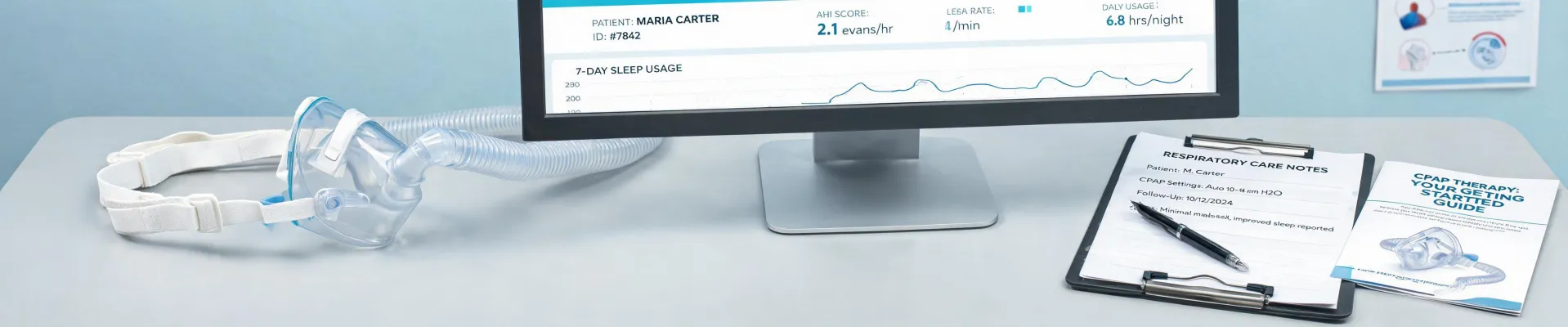
The real failure happens earlier. Most people don't realize that sleep apnea is one of the most common drivers of resistant hypertension. You can slap an ambulatory blood pressure monitor on someone for 24 hours and see wild swings—but if you never treat the root cause, those numbers will only get worse. That’s where tools like the My Air for Air 10 by ResMed app come in. It provides real-time adherence data, letting clinicians intervene before complications set in. That's the kind of loop that actually changes outcomes.
But the conversation is still dominated by rescue. When I train staff on defibrillator AED usage, I always emphasize: this is a response to failure. A good system should have a plan to avoid the cardiac arrest altogether—not just a drill for when it happens.
From my experience, the quiet stuff saves lives.
I once got a high-priority order for a ResMed AirSense 10 compatible mask—a rapid order turnaround that beat standard vendor track. The patient had severe sleep apnea, borderline heart failure, and his previous mask had a cheap seal failure. He ended up in emergency two days later. The mask wasn’t the problem—it was the lack of follow-up. So we implemented a policy: check mask compatibility at every visit and use the app to track compliance. Over the next quarter, readmissions dropped 12% for that patient group.
Now, what about the AED? Don’t get me wrong, I’m not against it. But if I have to choose between teaching someone how to use a defibrillator versus how to set up a CPAP and check if the mask seals properly, I know which one prevents more downstream disasters.
“Look, you can buy the loudest, shiniest emergency equipment—but what matters is what happens before the emergency. That’s where the system either works or it fails.”
I know the counterargument—sometimes you need both.
People tell me: “You can’t prevent everything. Heart attacks happen. Respiratory failure happens.” And that’s true. But I argue that if you invest heavily in prevention (like CPAP therapy, accessible sleep studies, and remote monitoring via the myAir app), you drastically reduce the frequency and severity of those events. One ambulatory blood pressure monitor result showing nighttime BP spikes is more actionable than a single emergency room BP reading—if you’ve got a team that acts on it.
A quick clarification, though, on monitoring: knowing how does a pulse oximeter work in a healthy person with mild desaturations can give false peace of mind. For a sleep apnea patient, that same device can show normal daytime oxygen—but the real damage happens when they're asleep. That’s why a CPAP with data logging is a better continuous monitor than a bedside oximeter without context.
And I’ll be honest—sometimes I second-guess myself. After I push a clinic to invest in more ResMed AirSense 10 compatible masks and a robust monitoring system, I wonder: “What if we missed something? What if a patient still needs an AED?” But then I check the data. In the centers we support with comprehensive CPAP programs, code blue calls drop. Not to zero—but noticeably. And the ones that do happen often involve patients who weren’t using CPAP in the first place.
Final thought: The best equipment in your practice isn’t the most expensive—it’s the one you use consistently.
So here’s my point: let’s stop acting like emergency equipment is the hero. Yes, a defibrillator AED saves lives. But so does a properly fitted mask and a clinician who checks in via an app before the patient has trouble breathing at night. If you’re designing a clinic workflow, build a prevention-first system: start with diagnosis (sleep study), then tools (CPAP, myAir app), then solid follow-up. Deploy the AED for the crashes, but work to prevent them.
That’s the opinion I hold after hundreds of projects. Simple.
Jane Smith
I’m Jane Smith, a senior content writer with over 15 years of experience in the packaging and printing industry. I specialize in writing about the latest trends, technologies, and best practices in packaging design, sustainability, and printing techniques. My goal is to help businesses understand complex printing processes and design solutions that enhance both product packaging and brand visibility.